
CHILD-BRIGHT has officially updated the language it uses to better represent the realities of our research partners. In this post, we explain:
how we arrived at these changes,
why we deemed them necessary, and
why language matters in health research.

How is CHILD-BRIGHT updating the language it uses?
CHILD-BRIGHT has made several updates to the terms it uses to describe engagement and its research partners:
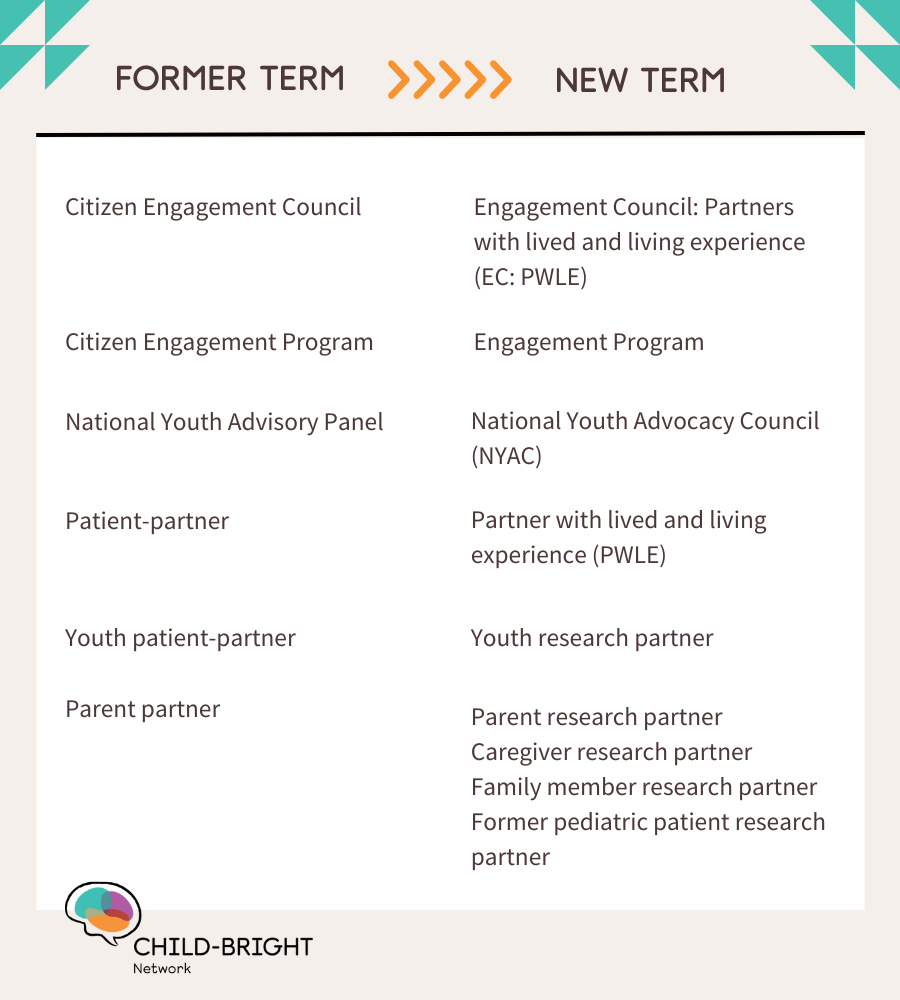
Download a plain-text version of this table
Why is CHILD-BRIGHT changing the vocabulary it uses to refer to its research partners?
Language has rules, but it is by no means static. The evolution of the vocabulary we use, both within and outside of childhood disability health research, reflects broader cultural shifts in how equity-seeking communities describe themselves, and how we perceive, interact with, and advocate for partners with lived and living experience (PWLEs) within our network. Over the past few months, we have engaged in an extensive consultation process, both with network members and the wider SPOR community, to adopt language that is more accurate, inclusive, and empowering to our youth and family research partners. This language refresh was spearheaded by our former Director of Engagement, Sharon McCarry.

Sharon McCarry
Former Director of Engagement
“When I joined CHILD-BRIGHT in 2021, one of the main things I wanted to work on was terminology,” says Sharon. Informal discussions around language, especially regarding the term ‘patient’, were ongoing within the network, but in 2023, Sharon saw an opportunity to move forward. CIHR had launched its SPOR Refresh exercise, which aimed to gather input on how to improve Canada's Strategy for Patient-Oriented Research. The year prior, CHILD-BRIGHT had also been successful in its application to the SPOR Networks – Knowledge Mobilization and Implementation Science competition, allowing us to begin moving our patient-oriented research into action through insight and methods grounded in implementation science and knowledge mobilization that embed the principles of equity, diversity, inclusion, decolonization and Indigenization (EDI-DI).
With change on the horizon, it was an ideal time to discuss the link between language and research partner engagement. Sharon knew that a language refresh would be complex but worthwhile. “When you take the first step, you’re the one everyone’s going to look at,” she says. “You need to have the courage to take the leap.”
How were these terms chosen?
Network members met at the 2023 CHILD-BRIGHT Conference to discuss moving away from certain terms, including ‘patient’ and ‘citizen engagement.’ ‘Patient,’ which has never been used to refer to First Nations, Métis, and Inuit community partners within the network, felt less and less applicable to our other partners with lived and living experience, as did ‘citizen’. In the months that followed, the network began a lengthy research and consultation process. With many diverse groups and key partners within CHILD-BRIGHT, varying perspectives needed to be heard. “I felt strongly that if labels were going to be considered, the very people that would be ‘labelled’ had to be included in that process,” says Sharon. “So, the exercise really became a grassroots effort.”

Logan Wong
Co-chair, National Youth Advocacy Council
From the start, feedback from CHILD-BRIGHT's youth members was integral. The network’s National Youth Advisory Panel decided on a revised name: the National Youth Advocacy Council (NYAC). NYAC member Sierra Lynne was steadfast about including the word ‘advocacy’ in the name, and his fellow council members agreed. “It represents us more authentically, because that’s what we are – we’re self-advocates,” says Logan Wong, co-chair of the NYAC. “We want to help children and youth with brain-based developmental disabilities have better experiences in the health care system than we did.”
Moving forward, CHILD-BRIGHT will use these new terms in all official documentation, with the exception of references to our First Nations, Métis and Inuit community partners, unless otherwise requested. We also recognize that there will never be perfect consensus on language, and we will always respect our research partners’ autonomy to use their preferred terms to identify or describe themselves.
“Our role as partners is more than sharing our diagnoses.”
Why does language matter when doing research about childhood disability?
The NYAC members were in favour of shifting from ‘patient’ to ‘partner with lived and living experience’. “None of us felt like we were patients,” says Logan. “The word always implied that we were connected to research through the medical system, but we aren’t sick, and our role as partners is more than sharing our diagnoses.”
In addition to these internal consultations, our Youth and Engagement Initiative Coordinator, Heather Muir, reviewed the public-facing language of other POR networks in Canada and abroad, and discussed terminology with SPOR-funded entities. Finally, CHILD-BRIGHT's new terms were reviewed multiple times by our Executive Committee.
CHILD-BRIGHT is proud to be the one of the first POR networks to make the leap and officially adopt this language. “I think these changes were necessary,” says Logan. “Language affects how we view disability and health in general. It can minimize stigma.”
Beyond terminology, CHILD-BRIGHT understands that there is more to be done to equitably engage people with lived and living experience as partners in POR.
“POR is relatively new,” says Sharon. “It’s only about ten years old.” She points out that the network can always do more to improve its inclusive practices. “A lot of education still needs to be done,” she says. “However, it’s very encouraging to see early career researchers leading the way in using inclusive language and practices in an authentic way. It is inspiring and gives me hope for change!”